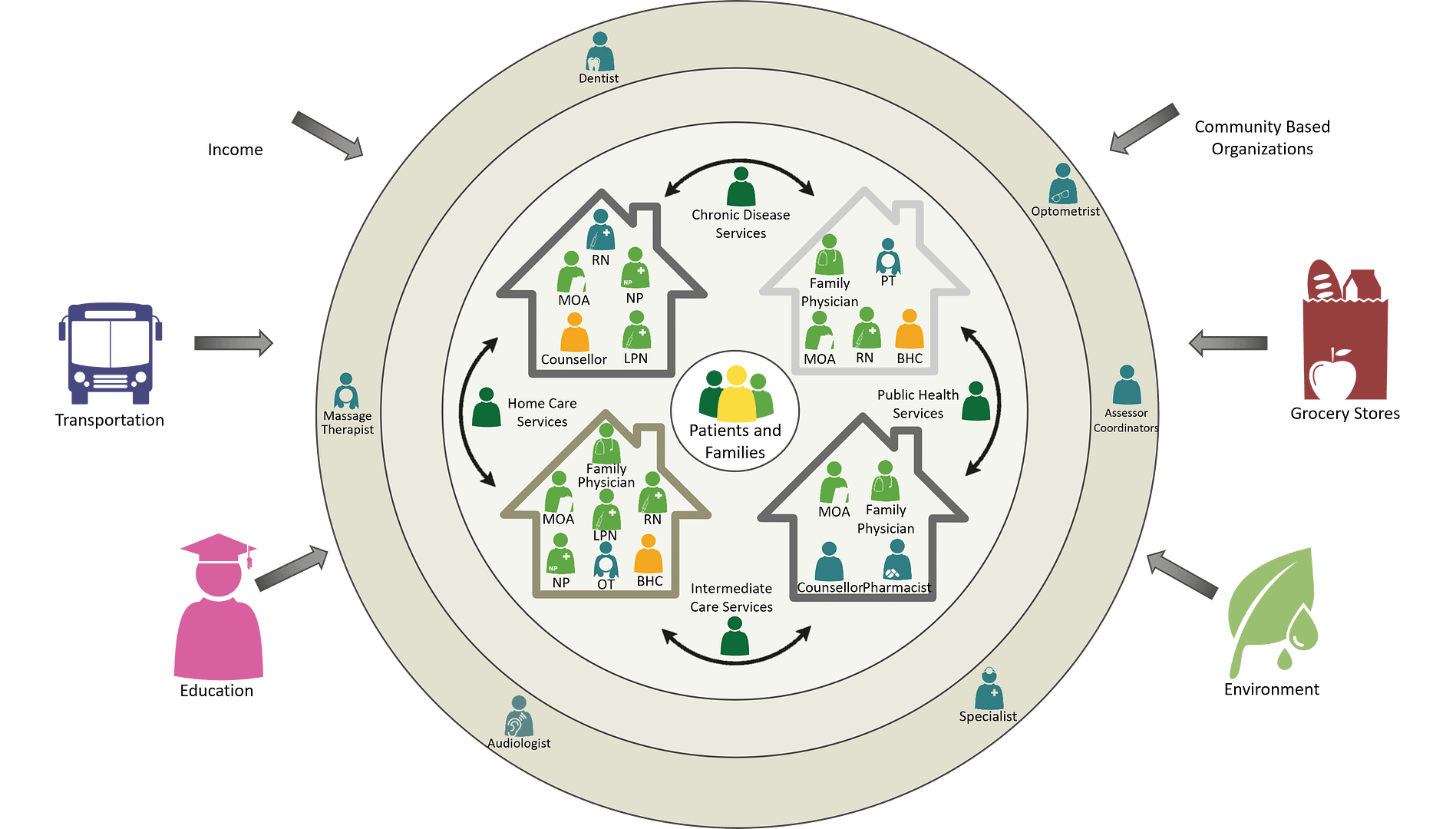
Saskatchewan’s healthcare system is evolving to ensure that every resident has access to comprehensive, tailored, high quality, team-based primary care through the development of Patient’s Medical Homes (PMH) in Health Networks. PMHs are family medicine clinics that provide patients with longitudinal, or continuous care across all life stages and are supported by a connected, interdisciplinary care team.
This work builds on our shared history in Saskatchewan of partnership between the SMA, SHA, and Ministry of Health to develop Health Networks as collaborative teams of health professionals, including physicians and community partners providing fully integrated services to meet the health needs of communities. This cross-organizational partnership to advance medical homes is unique across Canada, allowing us to leverage each of our strengths and resources to meet Saskatchewan peoples’ needs.
Collaboration between family physician clinics and the SHA is currently occurring in more than 150 clinics across Saskatchewan. The vision is to accelerate advancement of many more medical homes in health networks. The focus on Patient’s Medical Homes through strong partnership between the SMA, SHA, and Ministry of Health creates the conditions for significant advancement of the vision. Physician leadership at the clinic level is critical to ensure local decision making, problem solving and resourcing.
The PMH vision is well known across the country and is based on the College of Family Physicians of Canada’s work on an effective, interprofessional team-based model for family medicine. The PMH is a transformational change in service delivery that increases patient and provider satisfaction, improves quality of care, reduces cost, creates efficiency and reduces hospitalizations.
At the core of the vision is the physician and patient relationship – establishing a trusting, continuous long-term relationship for ongoing care throughout their life. This relationship may take time to build but is generally known to support better understanding of symptoms, answering questions, and reaching stronger health decisions and more positive health outcomes. The word ‘home’ is intentional, with PMHs built around the needs of patients where they feel the most comfortable discussing their personal, family health, and medical concerns.
Family Physician leadership is required in a Patient’s Medical Home.
For the PMH to continue to strengthen, Family Physician leadership is required. This is transformational work that requires a change in culture, relationships and routines. Engaged physician leaders are required to set the course as well as support and sustain efforts including at clinic, health network, and health system levels. Without engaged physician leaders, teams struggle to make and sustain key changes required for transformation. Within the PMH vision, engaged physician leaders should be visible throughout the transformation process.
At the clinic level, Family Physician leadership is one of the ‘must haves’ to strengthen the PMH vision. Family Physicians can demonstrate leadership by:
- Building physician leadership capacity
- Providing clinic direction and motivation to support a new way of working
- Developing and leading the team
- Learning more about your patient panel
- Deepening patient relationships
- Optimizing resources and operations
- Removing barriers and providing a supportive work environment for those working on the clinic’s transformation
- Continuously growing and improving to better meet the needs of patients
- Using technology support and health information data to inform decision-making
- Connecting with Health Network resources to navigate and connect patients and families to services within and outside the network, including community supports.
As the PMH model matures, teams grow and a broader range of services are offered by an interprofessional, physician-led team operating at or near the top of their scope of practice. The patient does not always see their family physician, but a high performing team functioning both within the clinic and within the Health Network ensures that patients are always seeing the right provider, at the right time.
In some clinics or localities, a Nurse Practitioner (NP) serves as the lead of the Patient’s Medical Home. Our vision is the NP would also be connected to a Family Physician on the team (virtually and/or in person).
PMHs & HNs are both needed and rely on each other to meet the needs of the clinic and community. As a high functioning system, they work together to support long-term relationships with patients, ensuring high quality, accessible team-based primary care in the community.
Health Networks are the structures used within the SHA, and beyond, to understand the needs of people in geographic areas (or communities) across the province and organize services and resources. Health Networks enable collaborative teams of health professionals, including physicians and community partners, to provide fully integrated services that meet the health needs of individuals and communities. Teams in Health Networks provide primary care (Family Physician type services) and primary health care (which includes disease prevention, public health, and broader health determinants). The delivery of primary health care is dependent on collaboration with all primary care clinics. Where strong collaboration exists, patient experience, patient outcomes, and health system efficiency improves.
Health Networks include physicians, nurse practitioners (NPs), nurses, allied health care providers, and other SHA (and non-SHA) service providers working collaboratively with each other and community organizations to provide all the primary health care services a local population requires. Through these networks, providers and community organizations collaborate to:
- Improve patient care using a team-based approach, supporting the right care by the right provider.
- Ensure patients are connected to the broader system and assist in navigating services for those that require assistance.
- Use data to determine the needs of the community and patient population, including tailored community programming for high-risk and vulnerable populations.
- Enhance patient access and attachment to primary care and reduce unnecessary use of acute and emergency services.
- Prevent ill health and promote wellbeing through disease prevention and management in accordance with leading practice (e.g., Clinical Pathways).
- Address the determinants of health and apply a health equity lens to improve population health outcomes.
SMA, SHA, and Ministry of Health collaborating to build the team in the clinic – where the patients are, in their medical home.
Currently, primary care is offered in different places, and most patients are referred to services outside of their Family Physician clinic – their Patient Medical Home – to see another healthcare provider. A common example is where a patient is referred to visit a Chronic Disease Nurse Educator, who works in a different facility. Patients are expected to wait for a call, are added to a waitlist and booked for an appointment, traveling to a separate location for sometimes disconnected services, away from the Family Physician and other team members.
The ideal change that we are striving to achieve is for the patient to be, “connected to care”, right within the Family Physician clinic, receiving continuous, accessible, team-based care, together with the right team members – their Patient’s Medical Home (in person or virtually). This change would result in the Chronic Disease Nurse visiting the patient in their Patient’s Medical Home clinic, thus enhancing integrated team-based care.
This change will take time to build and requires overcoming organizational silos and increased collaboration among healthcare partners. It also requires Shared Leadership among SMA, SHA, and Ministry of Health to coordinate team members, services and resources with Family Physicians and patients in clinics. This shared leadership to advance PMH in Health Networks is demonstrated among our health partners at several levels in the health system:
- Strategic Oversight: Policy and strategy level;
- Operational Oversight: Operations for PMHs in Health Networks level; and
- Local Oversight: Where the work occurs – at the local clinic level working with Health Network leadership.
The Innovation Fund is an opportunity to enhance our shared leadership between PMHs and the broader Health Network to transform how primary care is delivered.
The Saskatchewan Patient’s Medical Home Development Tool is available to help understand where your practice is at on the PMH development journey. It also outlines the next steps a clinic may choose to take to strengthen the Patient’s Medical Home vision in our province. There are four key areas of development:
- Engaged physician leadership and team functioning
- Patient-centered culturally responsive care
- Panels, measurement, and continuous quality improvement
- Care coordination and patient access
Patient’s Medical Home
- PMH Vision
- PMH Best Advice Guides that introduces key concepts for the Patient’s Medical Home Framework.
- A Saskatchewan PMH Development Tool is available to help understand where your practice is at on the PMH development journey.
- Saskatchewan College of Family Physicians Implementation Kit
Electronic Medical Record
Quality Improvement
- The Health Quality Council (HQC) Physician Panel Reports for Family Physicians.
- HQC QI in Clinics Program
Health Networks
- SHA Area Maps, Health Network map
- Health Network Profiles
- Use your SHA email to log in and view Health Network 101